



前回のお勉強は、私が何年もかけてお勉強して、研究した結果ができあがったオリジナルのIFの高い論文=医学博士主論文ですが、私は医師として美容医学(=形成外科・美容外科)に携わり、長年解明したく、精密な説を立てたかったので選んだテーマです。この論文をもって、私は美容医学博士と自称します。
今回画像を取り込めたので、前回の日本語抄訳に張り付けて説明します。英語文は必要部位だけにして、主に図の説明文を訳します。
Scanning Electron Microscopic Study on Double and Single Eyelids in Orientals
アジア人の二重まぶたと一重まぶたの走査式電子顕微鏡での研究;オリエンタルズを東アジア人と訳します。
Kazuhiko Morikawa, M.D., Hiroshi Yamamoto, M.D., Eiju Uchinuma, M.D., and Shohei Yamashina, M.D. Kitasato university, School of Medicine, Sagamihara, Japan
著者 森川一彦:主著者 山本博:共同研究者 内沼栄樹:北里大学形成外科・美容外科教授 山科正平:北里大学解剖学教室教授
Abstract:主張したい事はこの抄録に要約されています。抄録は前文ではなく、検索に使うために短文化した論旨です。
従来から、西洋人は挙筋腱膜の終末挿入が、眼瞼の前方にあるために二重まぶたであり、東洋人では、それがないため一重瞼になるというセオリーが提示されていた。しかし東洋人では、このセオリーで説明できない解剖的差異を示す報告がある。そのため、東洋人に置ける挙筋腱膜の走行を同定するため、日本人の眼瞼を走査式電子顕微鏡(SEM)を用いて観察した。3次元的な断面像によって二重瞼では西洋人の様に挙筋腱膜の枝、それも眼輪筋を貫いて繫がっているのを確認した。これは一重瞼では見られなかった。この新しい解剖的知見は、東洋人に置ける重瞼術のために重要な根本的基礎となると考えられる。
Key words: Oriental eyelid—Blepharoplasty—SEM
日本語文では、論旨を解りやすくするために起承転結で記述していく様に求められます。本論文のように洋語文でも、その形を採る事が多いのですが、前文(起)には名前がなく下段には標題があります。
前文の要旨:先ず私が言いたかったのは、西洋では(アジア人を対象としないという意味)、眼瞼形成術とはしわたるみ取り術が主で、アジアでは、重瞼術がしばしば行われること。したがって、この分野の手術はアジア人の解剖構造を知るべきだと考えられる。アジア人にも二重まぶたは存在する。二重まぶたと一重まぶたの解剖の報告は少ない。西洋人では挙筋腱膜が眼輪筋を貫き眼瞼の前葉に付着するのが二重瞼の構造だとされている。日本人でも、二重まぶたでは同様という説がある。引き換えて、二重まぶたと一重まぶたのではほかの要因もあるという説がある。例えば、挙筋腱膜と眼窩隔膜の合流する高さ。皮膚や皮下組織、眼輪筋、ROOF、瞼板前脂肪、眼窩脂肪の厚さなど。蒙古襞の程度。瞼板高や眼窩の深さの違いなどが報告されてきた。下線部は臨床的にも認められるが、重瞼には影響していない。他の構造的差異は臨床的には相関しない。また、挙筋腱膜の前葉への挿入はMRIでは見いだせないとの報告もあるが、挙筋腱膜の合流は皆同じだとし、前者の説を否定している。逆に最近の光学顕微鏡での研究で挙筋腱膜が前葉に付着する説を否定するものがある。そこでこの研究では、挙筋腱膜の走行を走査式電子顕微鏡で、日本人における二重まぶたと一重まぶたの解剖構造の差を明らかにするために行います。
Materials and Methods;検体と方法(承)は、さあ何をするかの説明です。今回の方法のポイントは、光学顕微鏡像と同様に眼瞼の断面を見るのですが、細胞成分を化学的に除去してから見るので、残ったコラーゲン繊維の走行を立体的に追えることです。細かい点は省きますが、これは定式の方法です。
Results
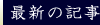
Light Microscopic Findings :Because the collagen fibers were well visualized by van Gieson’s stain, from the levator aponeurosis descending along the anterior surface of tarsus, branching off in the direction of the orbicularis oculi muscle anteriorly, the collagen fibers were shown to run into the muscle belly of the orbicularis oculi muscle. However, due to the thin sections, the view was interrupted, and we were unable to confirm whether or not the course of the collagen fibers was really continuous (Fig. 1 right side).
Scanning Electron Microscopic Findings: We were able to observe the direction of the levator aponeurosis, continuous with the levator palpebrae superioris muscle, using the SEM because it allows observation of cross-sections three dimensionally. It was easy to identify the levator palpebrae superioris muscle and Mu¨ller’s muscle posterosuperior to the conjunctival fornix by observing the directions of the bundle. By following the direction of these muscles towards the eyelid margin, we were able to detect each of the layers: the tarsus, aponeurosis, fat, and orbicularis oculi muscle (Fig.1 left side).
 Fig. 1. (Right) Light microscopic view. It seems that the levator aponeurosis branches anteriorly into the orbicularis oculi muscle (van Gieson’s stain, original magnification ×1). (Left) SEM view. White lines show each layer of the sagittal section of the eyelid (original magnification ×50). Mu¨ ; Mu¨ller’s muscle; LA ; levator aponeurosis; OF ; orbital fat.
Fig. 1. (Right) Light microscopic view. It seems that the levator aponeurosis branches anteriorly into the orbicularis oculi muscle (van Gieson’s stain, original magnification ×1). (Left) SEM view. White lines show each layer of the sagittal section of the eyelid (original magnification ×50). Mu¨ ; Mu¨ller’s muscle; LA ; levator aponeurosis; OF ; orbital fat.上図1は、右図が光学顕微鏡写真でファンギーソン染色というコラーゲンを赤く染める方法ですが、グレースケールでしかコピーできませんでした。オリジナルは1倍像です。挙筋腱膜が、眼輪筋に向かって前方に枝分かれしている。左図は走査電子顕微鏡(SEM)写真でオリジナルは50倍像です。図中の白線は矢状断出の各層を示しています。Mu;ミューラー筋 LA;挙筋腱膜 OF;眼窩脂肪
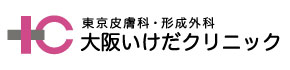
Furthermore, in order to identify the levator aponeurosis, we scanned and observed in the direction of the eyelid margin from the height of the upper margin of tarsus using high magnification. In samples of double eyelids obtained from cadavers, the levator aponeurosis was observed as a bundle of dense collagen fibers running in the same direction at the height of the upper margin of tarsus; it did not make contact with the tarsus until one-third of the height of the tarsus (Fig. 2).
 Fig. 2. (Upper) SEM view at the level of the upper one-third portion of tarsus of a double eyelid. White lines show each layer of eyelid. The levator aponeurosis runs down the anterior surface of the tarsus, and it has multiple lamella (original magnification ×50). T; Tarsus; Post; postaponeurotic fat. (Lower) A highly magnified view of the levator aponeurosis. This is formed by bundles of collagen fibers which run in the same direction and are dense (original magnification ×10,000).
Fig. 2. (Upper) SEM view at the level of the upper one-third portion of tarsus of a double eyelid. White lines show each layer of eyelid. The levator aponeurosis runs down the anterior surface of the tarsus, and it has multiple lamella (original magnification ×50). T; Tarsus; Post; postaponeurotic fat. (Lower) A highly magnified view of the levator aponeurosis. This is formed by bundles of collagen fibers which run in the same direction and are dense (original magnification ×10,000).上図2は、上半が50倍で見た二重まぶたの瞼板前の上1/3部のSEM像で、挙筋腱膜が瞼板の前面を下走しています。T;瞼板 Post;腱膜後脂肪 下半は同部の10,000倍という高拡大で見た挙筋腱膜像。これはコラーゲン繊維の束で出来ていて、同方向に走行し、密度が高い。
While this levator aponeurosis further ran inferiorly along the anterior surface of tarsus, a large number of collagen fiber branches could be seen running into the muscle belly of the orbicularis oculi muscle positioned anteriorly. In addition, the position in which the collagen fibers branch off was inferior to the orbital septum even at the highest position. These fibers were shown also by high magnification to be continuous with the levator aponeurosis anterior to the tarsus. High magnification also showed the branches to appear dense. Although there was slight disarray, the direction of the fibers was uniform, and similar to the fibers of the aponeurosis above (Fig. 3).
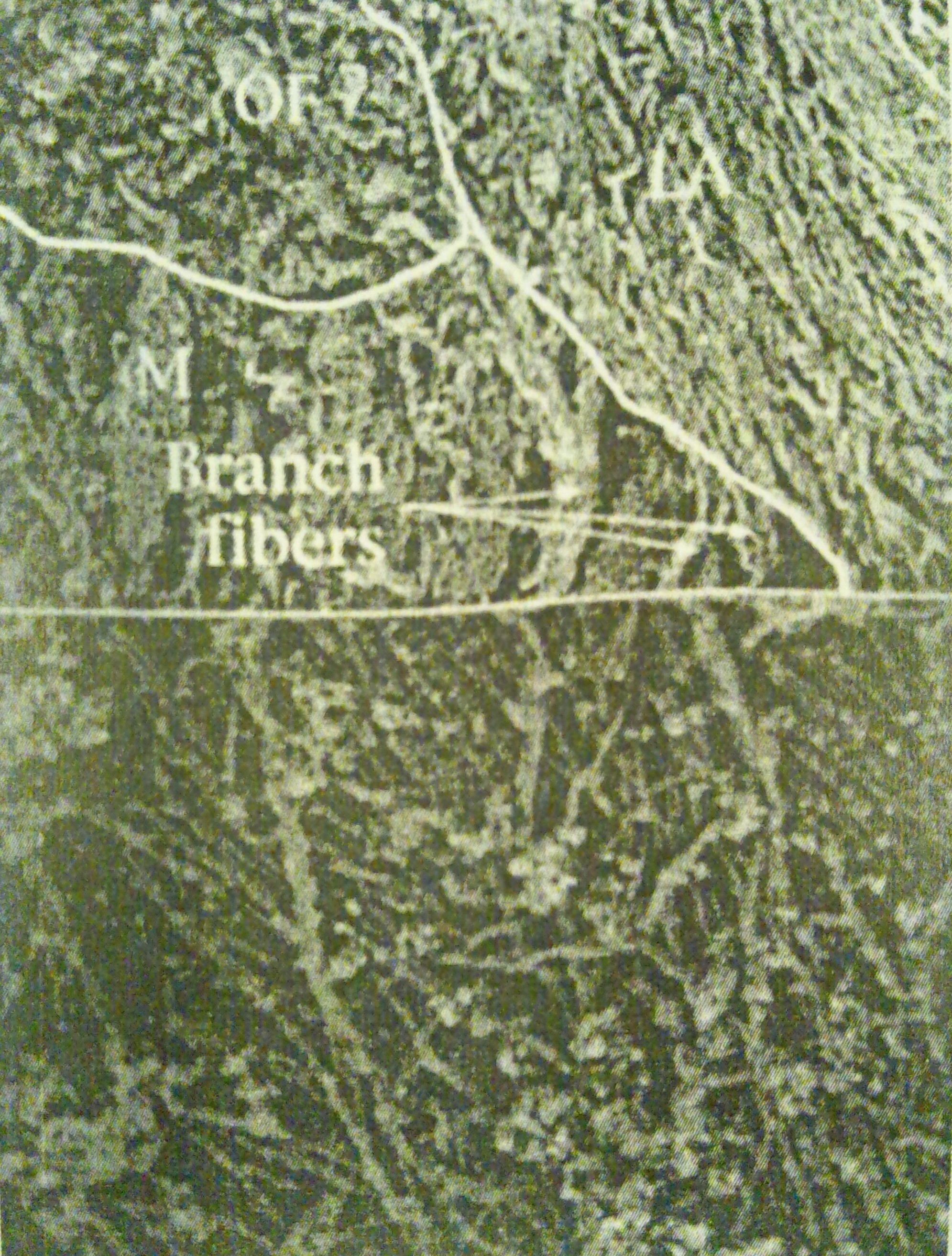 Fig. 3. (Upper) SEM view of the middle one-third portion of tarsus of the double eyelid. This shows the branch fibers of the levator aponeurosis that run between the bundles of fibers of the orbicularis oculi muscle. The fibers of the levator aponeurosis connecting the branch fibers (original magnification ×60). M ; orbicularis oculi muscle. (Lower) SEM highly magnified view of the branch fiber. The fiber is the same as in Figure 2 (original magnification ×10,000).
Fig. 3. (Upper) SEM view of the middle one-third portion of tarsus of the double eyelid. This shows the branch fibers of the levator aponeurosis that run between the bundles of fibers of the orbicularis oculi muscle. The fibers of the levator aponeurosis connecting the branch fibers (original magnification ×60). M ; orbicularis oculi muscle. (Lower) SEM highly magnified view of the branch fiber. The fiber is the same as in Figure 2 (original magnification ×10,000).上図3は、上半が60倍で見た二重まぶたの瞼板前の中1/3部のSEM像で、挙筋腱膜の枝の繊維が眼輪筋繊維の束の間を走行している。M;眼輪筋 下半は同部を10,000倍という高拡大で見た枝繊維の像。繊維は図2の挙筋腱膜と同様です。
Observation of the character and unidirection of the fibers suggested that the strength to open the eyelid is transmitted to the anterior portion similarly to the upper levator aponeurosis. This bundle of collagen fibers penetrates the orbicularis oculi muscle layer and inserts at the subcutaneous layer whereby it appears wavelike. This connects to collagen fibers that are not uniform in direction and are composed of subcutaneous connective tissue, but it does not reach the dermis (Fig. 4).
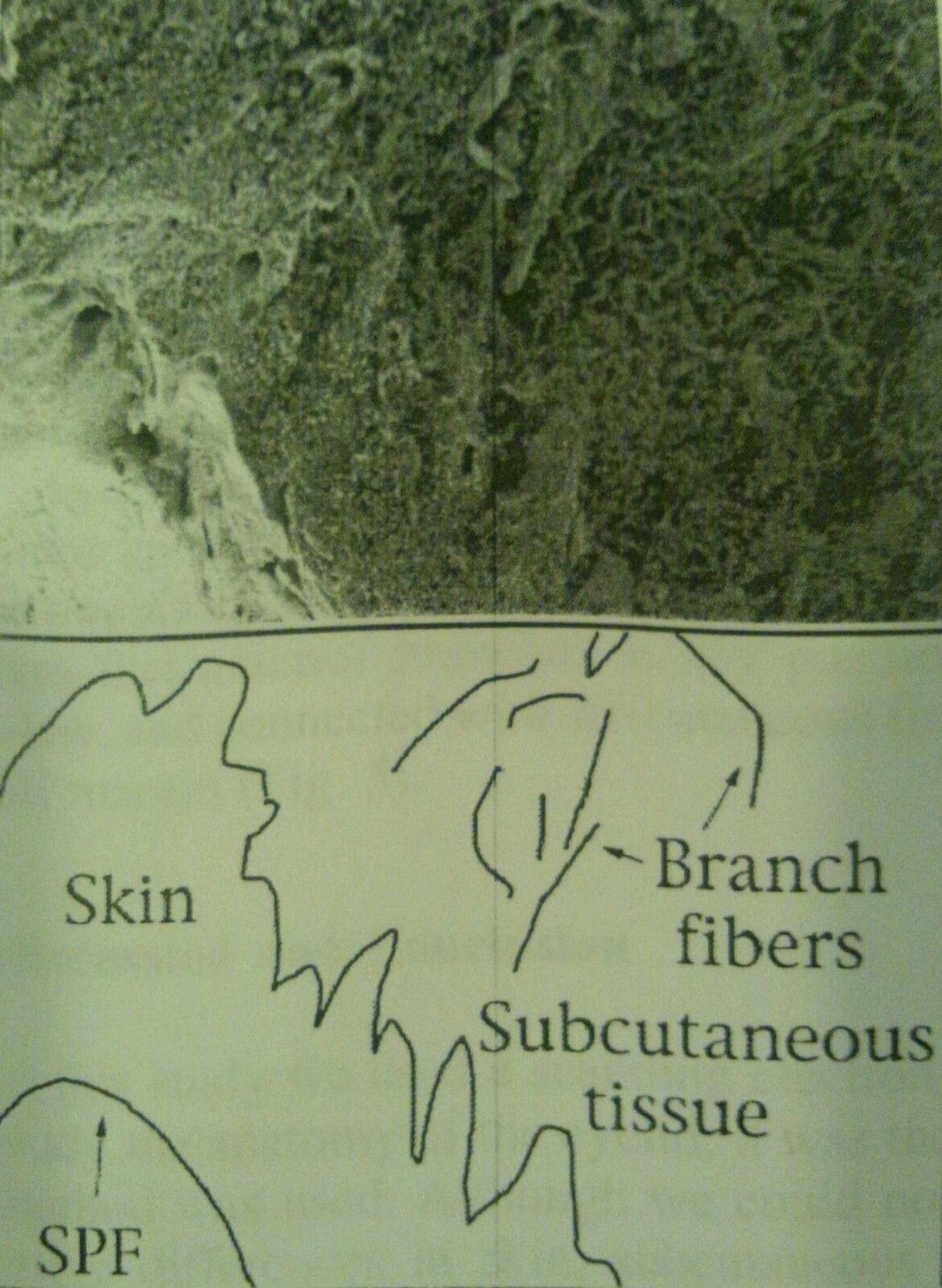 Fig. 4. SEM view of the eyelid margin. The schema shows that the branch fibers insert into the subcutaneous tissue. The supra palpebral fold is beneath this fiber (original magnification ×60).
Fig. 4. SEM view of the eyelid margin. The schema shows that the branch fibers insert into the subcutaneous tissue. The supra palpebral fold is beneath this fiber (original magnification ×60).上図4は、上半が60倍で見た眼瞼縁のSEM像。下半のシェーマ(模式図)は、枝分かれ繊維が皮下組織に挿入されるのを示している。上眼瞼溝(重瞼線のこと)はこの繊維の上層にある。
In single eyelids of cadavers, the direction of the levator aponeurosis anterior to the tarsus was the same as in double eyelids. But the difference with a double eyelid was that anterior branches at any position were out of view, and connected with subcutaneous tissue of the eyelid margin (Fig. 5).
 Fig. 5. (Upper) SEM view at the upper half portion of the tarsus of a single eyelid. The levator aponeurosis does not branch, and runs down for the eyelid margin (original magnification ×30). (Lower) SEM view of the lower half of the tarsus of a single eyelid. The levator aponeurosis inserts at the subcutaneous tissue and pretarsal connective tissue (original magnification ×30).
Fig. 5. (Upper) SEM view at the upper half portion of the tarsus of a single eyelid. The levator aponeurosis does not branch, and runs down for the eyelid margin (original magnification ×30). (Lower) SEM view of the lower half of the tarsus of a single eyelid. The levator aponeurosis inserts at the subcutaneous tissue and pretarsal connective tissue (original magnification ×30).上図5は、上半が30倍で見た一重瞼の瞼板前の上半部の像。挙筋腱膜は枝分かれしないで、瞼縁に向かって下走している。下半は30倍で見た一重瞼の瞼板前の下半部の像。挙筋腱膜は皮下組織や瞼板前の結合組織に挿入されている。
結果(転)はこうなりましたという事ですが、まだ何も主張していません。要約:二重まぶたでは、上眼瞼挙筋腱膜から密なコラーゲン繊維が前方に向かって枝分かれして走行し、眼窩脂肪の下を通って眼輪筋を貫いて、皮下組織に繋がっている。一重まぶたでは瞼縁まで枝分れがない。各図からいえることはこれだけです。
Discussion and Conclusion;今回図から得られた証拠が、考察されているので、各文を対訳します。
In this study we used a scanning electron microscope to study the anatomy of the eyelid; it was the first time this method was used.この研究では、走査電子顕微鏡で眼瞼の解剖を調べた。この方法は初めてである。 Although we could not study quantitative differences in skin, subcutaneous tissue, orbicularis oculi muscle, and fat, nor the positioning of fusion between the orbital septum and levator aponeurosis from the findings of the SEM, SEMでは量的な差異や癒合を調べられないが、we were able to view three dimensional images of the eyelid. 3次元的な像を提示できた。As a result, we were able to clarify the continuity of branch fibers of the levator aponeurosis. 結果として、挙筋腱膜の枝分かれ繊維の連続性を描出できた。When we investigated the double eyelid and single eyelid among Japanese, we found similarities with the findings of Sayoc [1] regarding the double eyelid. 日本人の二重瞼と一重瞼を検索したところ、二重瞼のセイヨックの説に合致した。That is, the bundle of collagen fibers that branch off from the levator aponeurosis run through the orbicularis oculi muscle layer and insert at the subcutaneous tissue layer. 挙筋腱膜より枝分かれしたコラーゲン繊維の束が眼輪筋を貫き走行し、皮下組織に挿入すると言う者です。However, in contrast to Sayoc’s findings, we found that this terminal fiber does not directly contact the skin, 直接皮膚に接していないが、but is continuous with the collagen fibers in subcutaneous tissue.皮下組織のコラーゲン繊維に連続していた。 It is thought that a double eyelid will result sufficiently even if this terminal fiber does not reach the dermis. 週末繊維が真皮に届いていなくても、二重瞼は確実にできると考えられる。In single eyelids, 一重瞼では、we observed that the levator aponeurosis runs along the tarsus inferiorly without branching off until the eyelid margin, and reaches the subcutaneous tissue of the eyelid margin.挙筋腱膜は瞼板に沿って下方へ枝分かれ無く瞼縁まで走行し、瞼縁の皮下組織に届くのを観察した。This result concerning the single eyelid was similar to previous reports. Whether or not the levator aponeurosis branches off below the orbital septum, passes through the orbicularis oculi muscle layer, and runs continuous with subcutaneous tissue is considered the determining factor for a double eyelid or a single eyelid (Fig. 6).この結果一重瞼は過去の報告と同様と示唆する。挙筋腱膜が、眼窩隔膜の下で枝分かれし、眼輪筋層を通過し、皮下組織に連続するかどうかが二重瞼と一重瞼を決定する要素と考えられる。図6
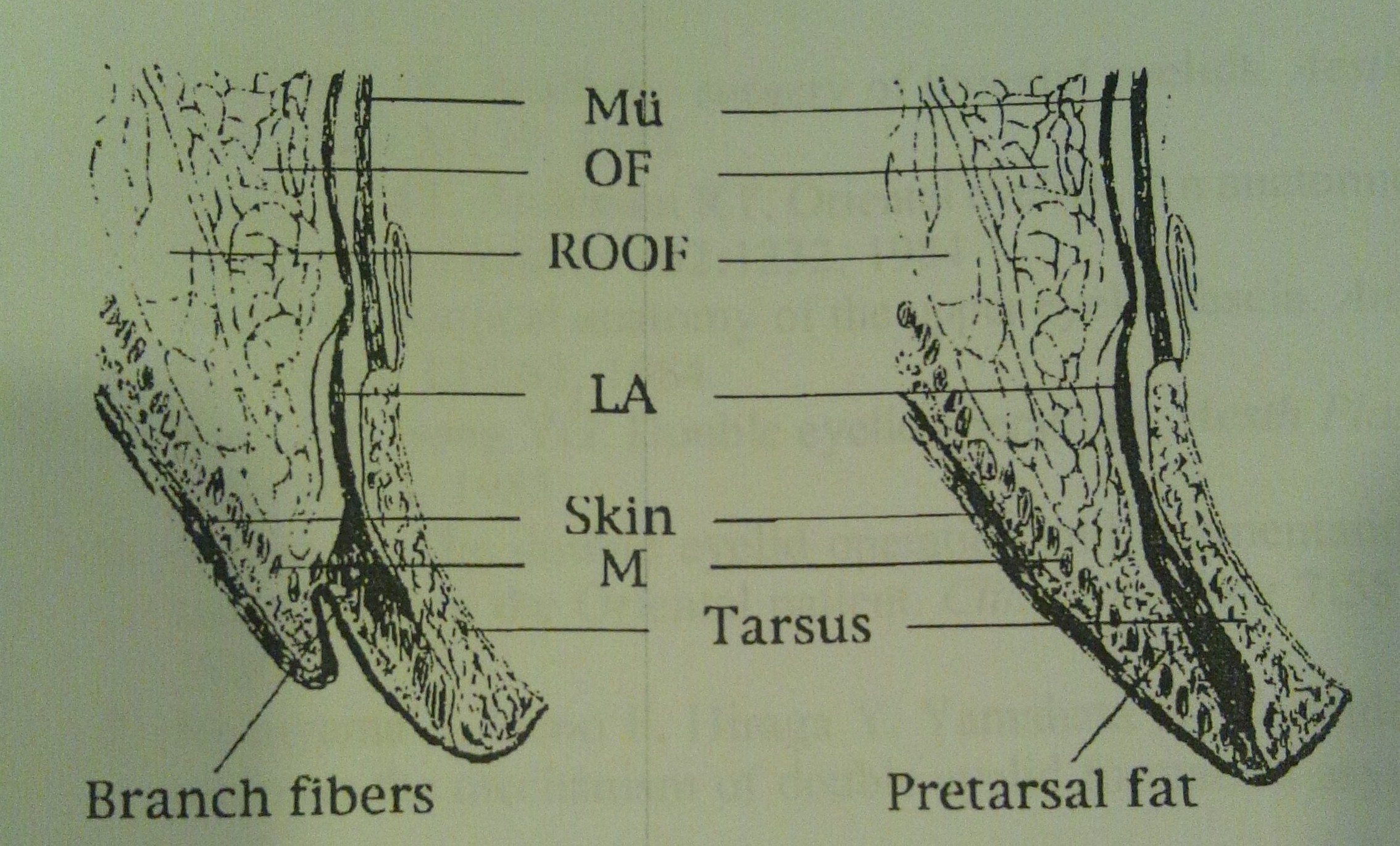 Fig. 6. Anatomic difference between a double eyelid (left) and a single eyelid (right) in an Oriental. The fundamental difference is whether or not there are branch fibers. Mu¨ ; Mu¨ller’s muscle;ROOF ; retro-orbicularis-oculi-fat; OF ; orbital fat;LA ; levator aponeurosis; M ; orbicular is oculi muscle.
Fig. 6. Anatomic difference between a double eyelid (left) and a single eyelid (right) in an Oriental. The fundamental difference is whether or not there are branch fibers. Mu¨ ; Mu¨ller’s muscle;ROOF ; retro-orbicularis-oculi-fat; OF ; orbital fat;LA ; levator aponeurosis; M ; orbicular is oculi muscle.上図6は、東洋人における二重瞼(左)と一重まぶた(右)の解剖的差異を示す。根本的な差異は、枝分かれの繊維があるかないかである。
Recently in Japan, there has been a report in which the authors could not find the insertion of the levator aponeurosis at the anterior portion by MRI [8], and a report in which fibers thought to be attached to the orbicularis oculi muscle were not continuous with the levator aponeurosis and did not extend to the dermis [9]. Sayoc’s theory, which explains the anatomical difference in eyelids between Occidentals and Orientals, has not been able to account for anatomical difference between double eyelids and single eyelids in Orientals. However, because a SEM, which we used, was more useful than other methods of investigation, it was possible to obtain clear results of the direction of the levator aponeurosis. We found that an important factor accounting for the anatomical difference between single eyelids and double eyelids in Orientals is the anatomical difference between the eyelids in Occidentals and Orientals reported by Sayoc. ここまではこれまでの説との対比で、ここからが結語です。Oriental aesthetic surgeons have many clinical opportunities to perform double eyelid operations to transform an Oriental single eyelid into a natural-looking Oriental double eyelid. In view of the results of the present histological study, we think that if double eyelid surgery is to be performed, it would be adequate if transmission of levator muscle force towards the anterior portion could be obtained by connecting a part of the levator aponeurosis with the most superficial layer of orbicularis oculi muscle, or by connecting a part of the levator aponeurosis with the most superficial layer of orbicularis oculi muscle and the subcutaneous tissue.
上記考察;西洋人は全員二重まぶたなのに、東洋人では二重まぶたと一重まぶたが混在している。両者は解剖構造の何が違うのかについて日本でもいくつか報告されていて、その中の一つには挙筋腱膜からの皮膚への連続性は認めなかったというものもある。しかし今回の走査電子顕微鏡による三次元的画像解析により、挙筋腱膜からの枝分れ繊維を描出できた。
結論としては:東洋の美容外科・形成外科医は、東洋人の一重まぶたを、自然に見える東洋人の二重瞼に改良する重瞼術を施行する機会が多い。ここに提示した組織学的研究の結果からの観点からして、重瞼術が施行されるならば、挙筋の一部が眼輪筋の最浅層か、皮下組織に連結するによって挙筋力が眼瞼前葉に向かって伝達されるようにすることが適切であると考える。
References
1. Sayoc BT: Absence of superior palpebral fold in slit eyes: An anatomic and physiological explanation. Am J Ophthalmol 42:298, 1956
2. Furukawa M: Aesthetic surgery of Oriental eyelids. Aesth Plast Surg 1:139, 1977
3. Doxanas MT, Anderson RT: Oriental eyelids. An anatomic study. Arch Ophthal 102:1232, 1984
4. Siegel R: Surgical anatomy of the upper eyelid fascia. Ann Plast Surg 13:263, 1984
5. Song RY, Song YG: Double eyelid operations. Aesth Plast Surg 9:173, 1985
6. Hiraga Y: The double eyelid operation and augmentation rhinoplasty in the Oriental patient. Clin Plast Surg 7:553, 1980
7. Nishiyama S, Ueno F, Hiraga Y, Yamahata A: Consideration on the mechanism of double eyelid formation asymmetry of the width in the double eyelid operation (Japanese). J Jpn Soc Aesth Plast Surg 11:67, 1989
8. Miyake I, Tange I, Hiraga Y: MRI findings of the upper eyelid and their relationship with single-and double-eyelid formation. Aesth Plast Surg 18:183, 1994
9. Tsurukiri K: Anatomy of upper lid (histological examination of a sagittal section through the upper lid-first report) (Japanese). Jpn J Plast Reconstr Surg 14:137, 1992
10. Ohtani O: Three-dimensional organization of the connective tissue fibers of the human pancreas: A scanning electron microscope study of NaOH-treated tissues. Arch Histol Jpn 50:557, 1987
ここには、参考文献として引用した事が示してあります。
Correspondence to Dr. Kazuhiko Morikawa, Department of Plastic and Reconstructive Surgery, Kitasato University School of Medicine, 1-15-1 kitasato, Sagamihara, Kanagawa 228- 8555, Japan. Aesth. Plast. Surg. 25:20–24, 2001
連絡先は、他の科学者からの反論や、参照時のコンタクトのために必要なのですが、連絡はありませんでした。他の形成外科医や美容外科医は興味がないのでしょうか?、それとも二重瞼と一重瞼の問題は世界人類の一部にしか関係ないからでしょうか?。実は論文の掲載誌のIFが低いからです。私はJSAPSに参加している日本の美容外科医約1000人のうちの200人とは毎年学会での情報交換していますが、この論文を読んでくれたのはそのうち10人に一人もいませんでした。重瞼術を行うのに興味ないなんて、なんて我が国の美容外科医は非科学的、ビジネス的なのかと、遺憾に思います。
DOI: 10.1007/s002660010088 © 2001 Springer-Verlag New York Inc.
これが、この論文の掲載誌の発行社です。多くの医学雑誌を刊行している会社です。
この論文は、美容外科医にとって基礎的な知識となると思います。上記の如く、二重瞼と一重瞼の解剖学的構造の違い3次元的に調べた結果を要説しました。美容外科医の皆さん、科学的論拠に則って美容医療をしようじゃありませんか?。糸で繋ぐだけでも切開するにしても、この議論の要旨は頭に入れておきましょう。そして美容医療を受ける患者樣方も、科学的根拠に基づいて診療を受けるために、最低限の知識としてこの論議を頭に入れておくといいと思います。